What began as a proposed Ebola isolation facility at Kenya’s Laikipia Air Base in Nanyuki is rapidly evolving into something much larger. It’s a test of public trust, clashing foreign policy, and the limits of government decision making in an increasingly informed society.
The U.S.-funded quarantine infrastructure has sparked protests, court action, and public debate. At first glance, this appears to be a public health issue. But a closer look suggests it may also be a foreign policy issue, one shaped by Kenya’s bilateral relationship with Washington, domestic political pressure, and growing public resistance to deals negotiated without enough transparency.
Why the United States and Kenya Are Cooperating on Ebola
The United States and Kenya have every reason to cooperate on Ebola preparedness. Ebola is currently spreading in Uganda and the Democratic Republic of Congo, where health professionals are working around the clock to contain the epidermic.
The consequences of an uncontrolled outbreak extend far beyond public health. Ebola can affect travel, trade, tourism, investment, and international mobility. Already the United States and other countries have restricted visas and travels from the affected countries to contain the spread of Ebola, something already disrupting business, air travel and tourism. The measure is aimed at preventing a repeat of the COVID 19 crisis that left millions of dead.
From a public health perspective, isolating exposed individuals within the region rather than transporting them across continents can make strategic sense. Epidemics require early containment, and the lessons of COVID-19 remind us how quickly diseases can spread through international travel. In that context, a regional Ebola isolation facility is not an unreasonable policy proposal.
The Bilateral Health Agreement Behind the Controversy
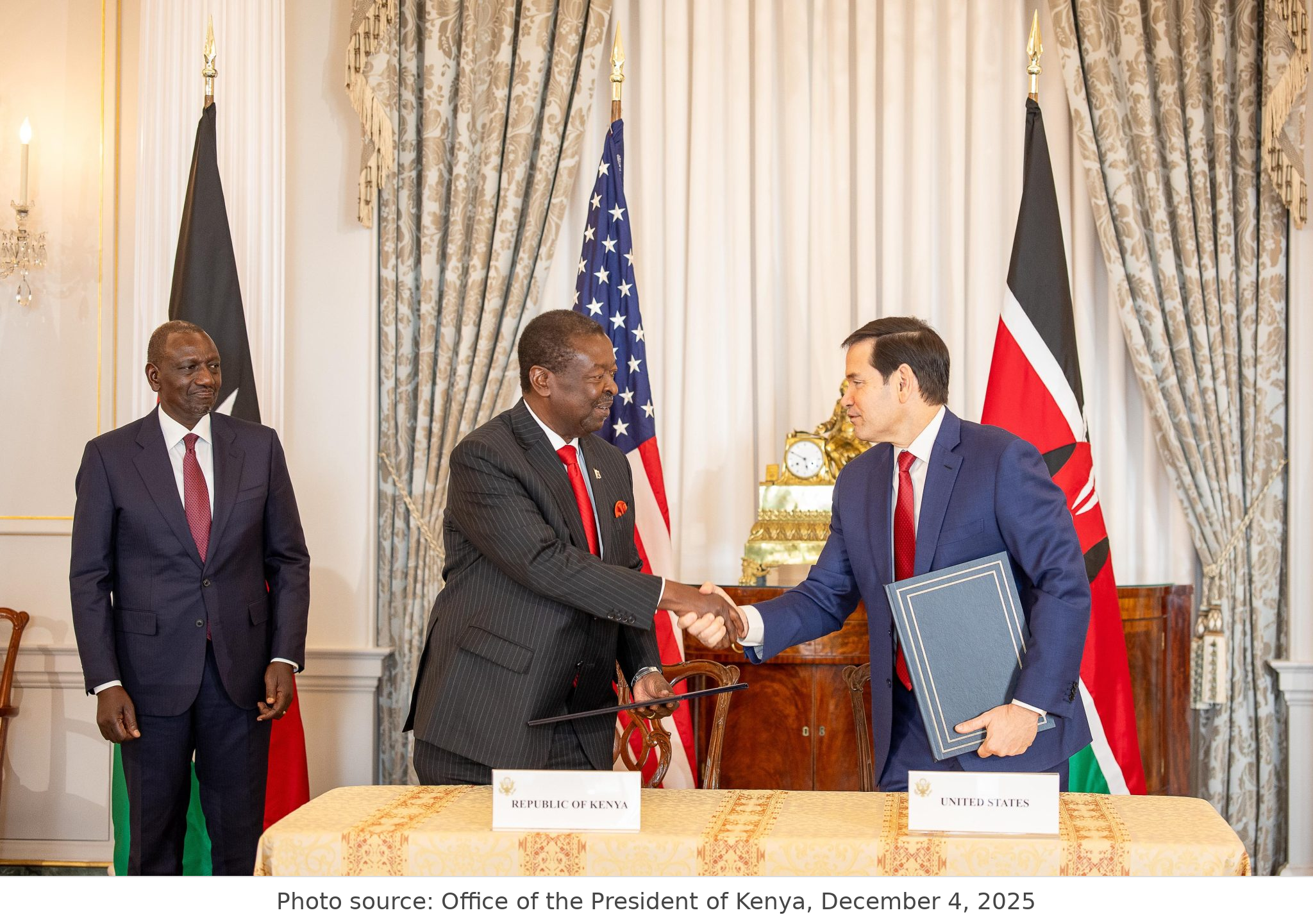
However, the proposed isolation center should also be understood within the broader United States-Kenya Health Cooperation Framework signed in December 2025. Under the five-year, $2.5 billion agreement, the United States committed up to $1.6 billion in health assistance while Kenya pledged to increase domestic health spending by $850 million.
Like most bilateral agreements, the framework advances both public health objectives and national interests. States provide assistance not only for humanitarian reasons, but also to advance strategic interests, strengthen partnerships, and promote policy objectives. It is within this broader framework that the proposed Ebola isolation center is now being pursued. But the project is also unfolding in the shadow of controversial Trump-era recalibrations of U.S. health and foreign policy toward Africa, where aid, security, disease preparedness, and national-interest calculations are increasingly being tied together. That wider context helps explain why the Nanyuki facility has attracted suspicion beyond its technical public-health purpose.
Why Nanyuki Became a Flashpoint
Many Kenyans are not asking only one question. They are asking several linked questions: If this facility is primarily intended for Americans exposed to Ebola in the region, what benefits does it bring to Kenya? What safeguards are in place for surrounding communities? What happens if an exposed person develops symptoms while in the country? Were local leaders and residents adequately informed? And why should Kenya host a facility that many citizens fear could expose them to risks created elsewhere?
Those concerns highlight a broader foreign policy challenge. Governments routinely enter into bilateral agreements without consulting every citizen. That is how diplomacy works. The policy problem for the Kenyan government is therefore not simply whether it had the authority to enter the arrangement. It likely did. The deeper challenge is whether it explained the public-health purpose, national benefit, and safety measures clearly enough before implementation, especially to the communities most likely to feel exposed by the decision.
A New Generation of Public Scrutiny
The protests also highlight how governance is changing in Kenya. Major policy decisions are no longer confined to government offices and diplomatic meeting rooms.
A politically aware and digitally connected generation is closely scrutinizing public policy and international agreements. Whether on taxation, governance reforms, or foreign-funded projects, Kenyan citizens, particularly Gen Z, have demonstrated a willingness to mobilize when they believe decisions affecting their future have been made without adequate public engagement.
In many developing countries, foreign-funded projects often become politically sensitive when citizens feel they were not adequately consulted. Whether those concerns are justified or not, perception matters. Public trust is a critical component of policy implementation.
Kenya’s Gains and the Unanswered Questions
The Kenya–U.S. health arrangement does answer part of the benefit question. The United States will provide $13.5 million toward Kenya’s Ebola preparedness, while Kenya’s government has defended the project as part of a wider emergency-response and public-health partnership. In principle, such cooperation can strengthen Kenya’s disease surveillance, laboratory testing, border screening, infection-control systems, emergency coordination, and the training of health workers. Kenya’s own Ministry of Health has also been emphasizing heightened Ebola preparedness, including surveillance, laboratory capacity, border screening, emergency response coordination, and public awareness.
The controversy, however, is not about whether Kenya should strengthen its health security. The real issue is whether the specific facility in Nanyuki is seen by local people as a Kenyan public-health investment or as a foreign risk-management site placed on Kenyan soil. Reuters has reported that the proposed unit at Laikipia Air Base in Nanyuki is a 50-bed quarantine facility intended for Americans who have been exposed to Ebola but are still asymptomatic. That distinction matters. To the U.S., the facility may be a preparedness measure. To many residents, it appears to be a plan to move the risk of Ebola exposure away from American territory and into a Kenyan community.
That is why the benefits must be explained in concrete terms, not only through diplomatic language. If the facility is part of a broader Kenya–U.S. health-security deal, then Kenyans need to know what will remain after the immediate Ebola concern passes. Will Laikipia County receive upgraded health infrastructure? Will Kenyan laboratories be strengthened? Will local hospitals and ambulance systems benefit? Will Kenyan health workers be trained and equipped? Will the country gain lasting capacity to detect, isolate, and respond to future outbreaks? If the answer is yes, those gains need to be clearly communicated and visibly delivered.
The disadvantage is not only the medical risk, especially if the facility is limited to people who are exposed but not yet symptomatic. The deeper disadvantage is political and social. Residents fear stigma, disruption to local business and tourism, inadequate consultation, and the possibility that a foreign government is being allowed to make sensitive public-health decisions without enough local consent. The anger has already turned deadly: protests in Nanyuki have led to reported deaths, arrests, and violent confrontations with police. A Kenyan court also ordered the temporary suspension of the plan after legal challenges raised concerns about public health and consultation, yet reports indicated that preparations and U.S. military activity around the site continued.
This is the heart of the dispute. The center is being built in the name of health security, but public trust has not kept pace with the project. Kenya may benefit from money, training, surveillance support, and emergency preparedness. But if citizens believe the country is being asked to host a risk that the United States does not want to bring home, the project becomes more than a health facility. It becomes a sovereignty issue, a transparency issue, and a test of whether international health partnerships can serve local communities as clearly as they serve foreign governments.
Policy Options for Moving Forward
First, the Kenyan government should do more to explain the public-health importance of the facility and how it fits into Kenya’s own preparedness needs. It is not enough to say the center is safe or that Ebola preparedness is necessary. Citizens need to understand why this facility matters, why Kenya is hosting it, how surrounding communities will be protected, and how the arrangement strengthens Kenya’s ability to respond to future outbreaks. The government does not need to disclose every diplomatic detail, but it must communicate the purpose, safeguards, and national benefit clearly enough to build public confidence.
Second, the United States should not support a facility on Kenyan soil that appears to serve only Americans during an Ebola outbreak. If the proposed center is built in Kenya, it should also be visibly linked to Kenya’s own public-health needs and accessible benefit. It should strengthen the country’s ability to provide high-quality preventive, emergency, and life-saving services for Kenyans who may be affected by Ebola or other dangerous infectious diseases.
This means the project should not be seen merely as a quarantine site for asymptomatic Americans exposed elsewhere. It should be tied to lasting investments in Kenya’s health system, including laboratory capacity, disease surveillance, infection-control equipment, emergency response systems, isolation capacity, technology transfer, and training for Kenyan health professionals. A facility built in Kenya should leave Kenya better prepared, not simply provide Washington with an offshore solution for managing its own exposure risk.
Third, civil society and citizens should continue demanding transparency and accountability, but they should not be only reactionary or oppose the facility for the sake of opposition. Ebola remains a legitimate regional public-health and security threat that requires preparedness, cooperation, and serious policy discussion. The role of civil society should be to push both governments to explain the project clearly, disclose the safeguards, and demonstrate how Kenya will benefit.
At the same time, public anger should be matched with constructive engagement. Civil society, health experts, community leaders, and residents should weigh the long-term benefits of the facility against the possible disadvantages, including health fears, stigma, public trust, and local disruption. If the facility can strengthen Kenya’s disease surveillance, emergency response, laboratory capacity, and health-worker training, those benefits should be examined seriously. The goal should not be blind acceptance or automatic rejection, but an informed national conversation about whether the arrangement protects Kenya’s interests as well as public health.
Fourth, Kenya and the United States should have held a joint press conference to address public concerns directly. For a project involving Ebola, a foreign-backed facility, and a host community already on edge, a press release is not enough. Journalists could have asked questions on behalf of citizens about the purpose of the facility, the safeguards in place, the benefits to Kenya, and the limits of the arrangement.
Such direct communication may not have removed every concern, but it could have reduced confusion, corrected misinformation, and possibly prevented public anger from escalating into protests.
Beyond Ebola: The Real Debate
Tensions remain in Nanyuki, but the real debate extends beyond the proposed Ebola isolation facility. Public anger appears to be rooted in a broader health cooperation deal that has raised questions about data sharing, sovereignty, and the changing terms of U.S. foreign policy in Africa.
Under this new approach, health assistance is no longer viewed only as aid. It is increasingly tied to strategic interests, emergency preparedness, and the protection of American citizens in the region. For many Kenyans, the concern is not simply that an Ebola facility may be built on Kenyan soil. It is whether Kenya is being asked to absorb public health risks while the terms, benefits, and safeguards of the agreement remain unclear.
Ebola may be the trigger, but the debate now extends far beyond disease control. At its core, this controversy reflects broader questions about sovereignty, transparency, public participation, and how governments communicate complex international agreements to their citizens.
The outcome of this dispute may ultimately shape not only Kenya’s approach to public health cooperation, but also public confidence in future bilateral agreements with international partners.



A very insightful analysis!